高プロラクチン血症
ドパミンはプロラクチン放出を阻害するため,ドパミン拮抗薬は血漿中プロラクチン濃度を上昇させると予測される。プロラクチン上昇の程度は用量に関連すると考えられ1,ほとんどの薬剤でのプロラクチン増加の閾値活性(ドパミンD2受容体占有率)は治療域に非常に近い2。遺伝的差異も関係があると考えられる3。表1.29にプロラクチン濃度に対する影響に従って各抗精神病薬をグループ分けする。
表1.29 抗精神病薬がプロラクチン濃度に及ぼす影響4–11
| プロラクチン濃度上昇を伴いにくい(プロラクチン濃度上昇は非常に稀) | プロラクチン濃度を上昇させる(低リスク,軽微な変化のみ) | プロラクチン濃度を上昇させる(高リスク,大幅な変化をもたらす) |
| アリピプラゾール | ルラシドン | amisulpride |
| アセナピン | オランザピン | パリペリドン |
| ブレクスピプラゾール | ziprasidone | リスペリドン |
| cariprazine | スルピリド | |
| クロザピン | FGA | |
| iloperidone | ||
| lumateperone | ||
| pimavanserin | ||
| クエチアピン |
高プロラクチン血症は,表面的には無症状であることが多いため(患者が自発的に問題を報告することはない),主観的QOLには影響しないというエビデンスがいくつかある12。しかし,血漿中プロラクチンの持続的上昇は視床下部-下垂体-生殖腺系の抑制を招く13。例えば,性機能障害14(他の薬理学的作用による場合もあることに注意する15),月経障害4, 16,乳房肥大と乳汁漏出16があり,妊娠妄想17も含めてよいかもしれない。長期的には,骨密度減少18, 19および乳癌リスク上昇の可能性20にもつながる。
プロラクチンはストレス,妊娠および授乳,けいれん発作,腎機能障害,その他プロラクチノーマ等の身体状態7, 21, 22によっても上昇する。プロラクチンを測定する場合,サンプルは早朝に採取し,静脈穿刺中のストレスを最小限にすべきである22。
禁忌
以下に該当する場合は,可能であればプロラクチン濃度を上昇させるリスクが高い薬剤の投与を避ける。
- 25歳未満の患者(最大骨量への到達前)
- 骨粗鬆症を有する患者
- ホルモン依存性乳癌の既往がある患者
- 若年女性
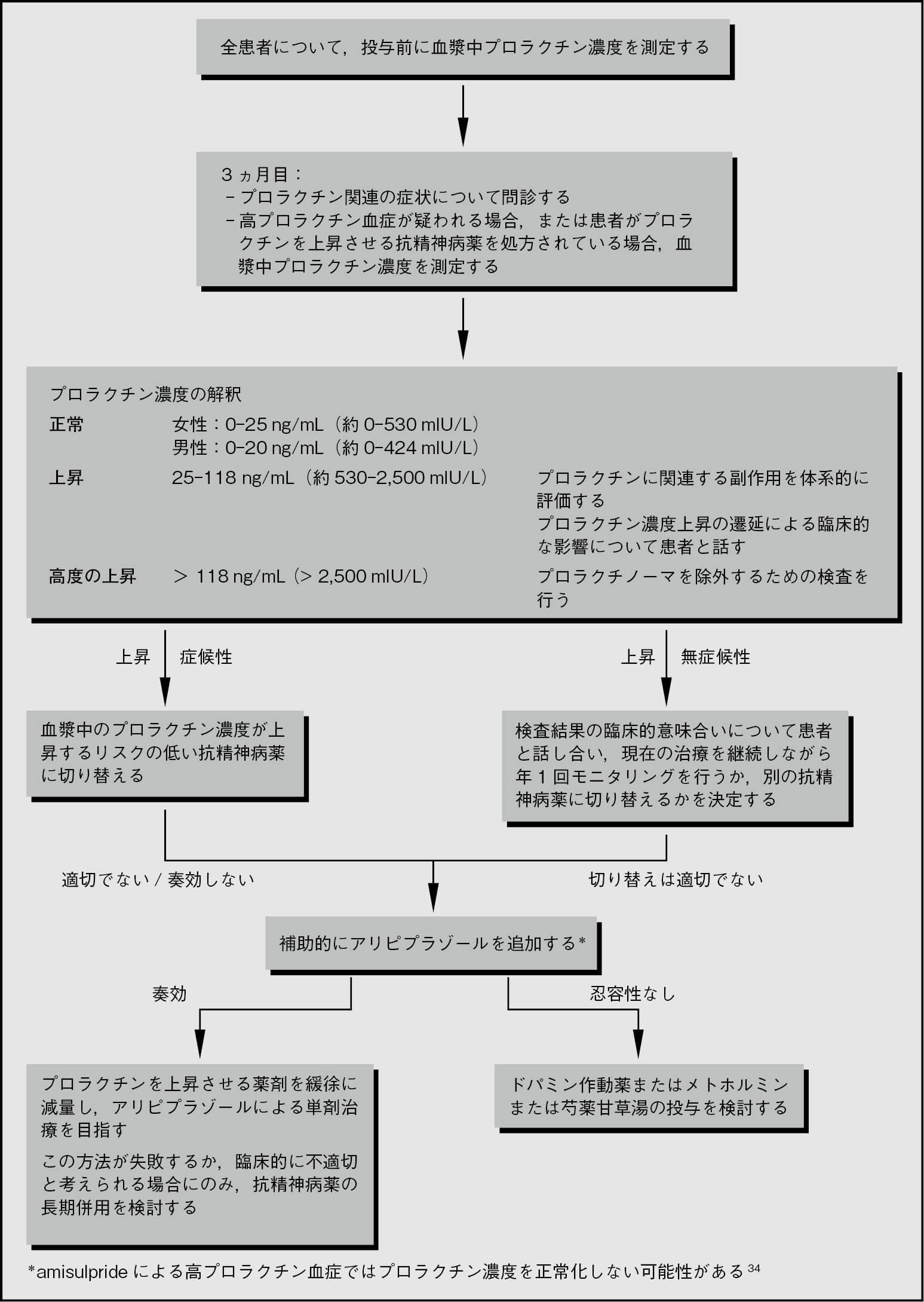
管理(図1.3)
高プロラクチン血症の治療は,血漿中プロラクチン濃度の測定値よりも症状と長期的リスクに応じて決定する。
以下に,抗精神病薬による高プロラクチン血症の管理のアルゴリズムを提案する。高プロラクチン血症の治療が必要である場合,プロラクチン濃度を上昇させない抗精神病薬への切り替えが第一選択であるが,切り替えは常に疾患の不安定化と再発のリスクを招く23。代替法はアリピプラゾールを既存の治療に追加することである24。アリピプラゾールは用量依存的にプロラクチン濃度を低下させる。3mg/日で効果があるが,6mg/日ではさらなる効果が期待できる。これ以上の用量は必要ないようである25。骨密度に対する長期的リスクを低下させるその他の戦略も議論すべきであろう(例:禁煙,体重負荷運動の増加,十分なカルシウムおよびビタミンD3の摂取18, 26)。
プロラクチンを上昇させる抗精神病薬を続ける必要がある場合や,アリピプラゾールに忍容性がない場合には,ドパミン作動薬が有効である可能性がある27-29。アマンタジン,カベルゴリン,ブロモクリプチンが使用されているが,少なくとも理論的には,いずれも精神病症状を増悪させる可能性がある(しかし臨床試験では報告されていない)。漢方(芍薬甘草湯)もプロラクチン関連症状に有効であることが示されているが30, 31,データは少ない。抗精神病薬を投薬中の糖尿病女性を対象とした研究において,高用量(2.5-3g)メトホルミン32の連日投与によりプロラクチン濃度も低下した。
図1.3 抗精神病薬による高プロラクチン血症の管理33
治療法の要約
| 第一選択 | アリピプラゾール5mg/日 |
| 第二選択 (優先順位ではない) |
DA作動薬:カベルゴリン,ブロモクリプチン,アマンタジン 芍薬甘草湯 メトホルミン2.5-3g/日 |
(水島 仁)
参照文献
- Suzuki Y, et al. Differences in plasma prolactin levels in patients with schizophrenia treated on monotherapy with five second-generation antipsychotics. Schizophr Res 2013; 145:116–119.
- Tsuboi T, et al. Hyperprolactinemia and estimated dopamine D2 receptor occupancy in patients with schizophrenia: analysis of the CATIE data. Prog Neuropsychopharmacol Biol Psychiatry 2013; 45:178–182.
- Young RM, et al. Prolactin levels in antipsychotic treatment of patients with schizophrenia carrying the DRD2*A1 allele. Br J Psychiatry 2004; 185:147–151.
- Haddad PM, et al. Antipsychotic-induced hyperprolactinaemia: mechanisms, clinical features and management. Drugs 2004; 64:2291–2314.
- Holt RI, et al. Antipsychotics and hyperprolactinaemia: mechanisms, consequences and management. Clin Endocrinol 2011; 74:141–147.
- Leucht S, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. Lancet 2013; 382:951–962.
- Peuskens J, et al. The effects of novel and newly approved antipsychotics on serum prolactin levels: a comprehensive review. CNS Drugs 2014; 28:421–453.
- Citrome L. Cariprazine: chemistry, pharmacodynamics, pharmacokinetics, and metabolism, clinical efficacy, safety, and tolerability. Exp Opin Drug Metab Toxicol 2013; 9:193–206.
- Marder SR, et al. Brexpiprazole in patients with schizophrenia: overview of short- and long-term phase 3 controlled studies. Acta Neuropsychiatr 2017; 29:278–290.
- Vanover KE, et al. Dopamine D(2) receptor occupancy of lumateperone (ITI-007): a positron emission tomography study in patients with schizophrenia. Neuropsychopharmacology 2019; 44:598–605.
- Yunusa I, et al. Pimavanserin: a novel antipsychotic with potentials to address an unmet need of older adults with dementia-related psychosis. Front Pharmacol 2020; 11:87.
- Kaneda Y. The impact of prolactin elevation with antipsychotic medications on subjective quality of life in patients with schizophrenia. Clin Neuropharmacol 2003; 26:182–184.
- Smith S, et al. The effects of antipsychotic-induced hyperprolactinaemia on the hypothalamic-pituitary-gonadal axis. J Clin Psychopharmacol 2002; 22:109–114.
- De Hert M, et al. Second-generation and newly approved antipsychotics, serum prolactin levels and sexual dysfunctions: a critical literature review. Exp Opin Drug Saf 2014; 13:605–624.
- Baldwin D, et al. Sexual side-effects of antidepressant and antipsychotic drugs. Adv Psychiatric Treat 2003; 9:202–210.
- Wieck A, et al. Antipsychotic-induced hyperprolactinaemia in women: pathophysiology, severity and consequences. Selective literature review. Br J Psychiatry 2003; 182:199–204.
- Ali JA, et al. Delusions of pregnancy associated with increased prolactin concentrations produced by antipsychotic treatment. Int J Neuropsychopharmacol 2003; 6:111–115.
- De Hert M, et al. Relationship between antipsychotic medication, serum prolactin levels and osteoporosis/osteoporotic fractures in patients with schizophrenia: a critical literature review. Exp Opin Drug Saf 2016; 15:809–823.
- Tseng PT, et al. Bone mineral density in schizophrenia: an update of current meta-analysis and literature review under guideline of PRISMA. Medicine 2015; 94:e1967.
- De Hert M, et al. Relationship between prolactin, breast cancer risk, and antipsychotics in patients with schizophrenia: a critical review. Acta Psychiatr Scand 2016; 133:5–22.
- Holt RI. Medical causes and consequences of hyperprolactinaemia. A context for psychiatrists. J Psychopharmacology 2008; 22:28–37.
- Melmed S, et al. Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2011; 96:273–288.
- Montejo AL, et al. Multidisciplinary consensus on the therapeutic recommendations for iatrogenic hyperprolactinemia secondary to antipsychotics. Front Neuroendocrinol 2017; 45:25–34.
- Sá Esteves P, et al. Low doses of adjunctive aripiprazole as treatment for antipsychotic-induced hyperprolactinemia: a literature review. Eur Psychiatry 2015; 30 Suppl 1:393.
- Yasui-Furukori N, et al. Dose-dependent effects of adjunctive treatment with aripiprazole on hyperprolactinemia induced by risperidone in female patients with schizophrenia. J Clin Psychopharmacol 2010; 30:596–599.
- Meaney AM, et al. Bone mineral density changes over a year in young females with schizophrenia: relationship to medication and endocrine variables. Schizophr Res 2007; 93:136–143.
- Hamner MB, et al. Hyperprolactinaemia in antipsychotic-treated patients: guidelines for avoidance and management. CNS Drugs 1998; 10:209–222.
- Duncan D, et al. Treatment of psychotropic-induced hyperprolactinaemia. Psychiatric Bulletin 1995; 19:755–757.
- Cavallaro R, et al. Cabergoline treatment of risperidone-induced hyperprolactinemia: a pilot study. J Clin Psychiatry 2004; 65:187–190.
- Yuan HN, et al. A randomized, crossover comparison of herbal medicine and bromocriptine against risperidone-induced hyperprolactinemia in patients with schizophrenia. J Clin Psychopharmacol 2008; 28:264–370.
- Man SC, et al. Peony-glycyrrhiza decoction for antipsychotic-related hyperprolactinemia in women with schizophrenia: a randomized controlled trial. J Clin Psychopharmacol 2016; 36:572–579.
- Krysiak R, et al. The effect of metformin on prolactin levels in patients with drug-induced hyperprolactinemia. Eur J Intern Med 2016; 30:94–98.
- Walters J, et al. Clinical questions and uncertainty–prolactin measurement in patients with schizophrenia and bipolar disorder. J Psychopharmacology 2008; 22:82–89.
- Chen CK, et al. Differential add-on effects of aripiprazole in resolving hyperprolactinemia induced by risperidone in comparison to benzamide antipsychotics. Prog Neuropsychopharmacol Biol Psychiatry 2010; 34:1495–1499.