緊張病
緊張病には,精神運動行動が低下する遅滞または昏迷型と,激越,攻撃性,衝動性,無目的に見える過活動性を特徴とする興奮型の2つのサブタイプがある1, 2。昏迷型は昏迷として現れる傾向があり,主要な特徴は無言症,筋強剛,著明な精神運動の遅滞,拒絶症,姿勢保持,蠟屈症,カタレプシー等である。昏迷は古くから統合失調症に関連するとされてきたが,うつ病や,それより頻度は低いが躁病3-8,アルコール離脱9,ベンゾジアゼピン系薬剤離脱10,転換性障害3, 4, 11-17等のその他の精神疾患でもみられる。精神疾患による昏迷を治療しないと必ず身体的な合併症が生じ,急速に悪化する。脱水,静脈血栓症,肺塞栓症,肺炎等の重篤な合併症,最終的には死亡を予防するために,迅速な治療が非常に重要である18。
緊張症候群は,自閉症等の発達障害,神経変性疾患19, 20や以下の疾患を含む,様々な全身性疾患,神経疾患,中毒性疾患によって生じる可能性がある。
- くも膜下出血
- 大脳基底核障害
- 非けいれん性てんかん重積状態
- 閉じ込め症候群,無動無言症
- 内分泌・代謝疾患(例:Wilson病)21
- Prader-Willi症候群
- 抗リン脂質抗体症候群22
- 自己免疫性脳炎23
- 全身性エリテマトーデス24
- 感染症(特にCNS感染症)
- 認知症
- 薬剤を中止した状態や薬剤に毒性がある状態。例えば,クロザピンの突然の中断やゾルピデム,ベンゾジアゼピン系薬剤25の中断が原因になる場合もあり,がん領域の薬剤等,向精神薬以外の薬剤が原因の場合も多い。
緊張病における昏迷の治療法は原因にある程度基づくが,通常,ベンゾジアゼピン系薬剤を含めるべきである。気分障害や転換性障害によって昏迷が生じた場合には,ベンゾジアゼピン系薬剤単独が治療選択肢となる5, 6, 26。ベンゾジアゼピン系薬剤はGABA作動性伝達を増加させ,脳由来神経栄養因子のレベルを下げると考えられる27。ロラゼパムに関する臨床経験が最も多い。多くの患者は標準用量(最大4mg/日)で反応するが,高用量(8-24mg/日)を繰り返し投与しなければならない場合もある28。気分障害(大うつ病性障害または双極性障害)を背景に緊張病性昏迷を呈した患者を対象に,ロラゼパム-ジアゼパム投与法を用いた小規模観察研究5では,ロラゼパム2-4mgを筋肉内投与した患者12例中10例において反応が認められた。極めて類似した投与法を用いた別の研究では,一般身体疾患または物質乱用に起因する緊張病を有する患者21例中18例において,症状の緩和が認められた29。ベンゾジアゼピン系薬剤が有効であれば,その効果は迅速に現れる。ゾルピデムの試験用量(10mg)により,ベンゾジアゼピン系薬剤に対する反応を予測できる可能性があり30,ゾルピデムの頻回投与は有効な治療となるかもしれない31, 32。ロラゼパムの静脈内投与も,反応の予測に用いられている33。
統合失調症の緊張病はベンゾジアゼピン系薬剤単独に反応しにくい可能性があり,反応がみられるのは症例の40-50%である34。ロラゼパムを最大で6mg/日投与した二重盲検プラセボ対照クロスオーバー試験では,統合失調症と確定診断された患者の慢性緊張病症状に対する効果は認められず35,ロラゼパムがあまり効果を示さなかった非無作為化試験36の結果と同様であった。コクラン・レビュー37では,統合失調症や類似する重篤な精神疾患(SMI)の患者の緊張病に対してベンゾジアゼピン系薬剤の投与または別の関連する治療を行ったRCTを検索した。適格したのは,ロラゼパムまたはoxazepamを投与した患者17例を対象とした1件の研究のみであり,効果に明確な差は認められなかった。ベンゾジアゼピン系薬剤をプラセボまたは標準治療と比較したデータは得られなかったことを,著者らは注記している。
統合失調症では,錐体外路副作用や神経遮断薬悪性症候群(NMS)等の鑑別診断がさらに問題を複雑にしている。精神病における緊張病性昏迷とNMSの類似点と相違点については議論が続いている38-41。自律神経の不安定性と高熱を伴う昏迷を表す言葉として,致死的緊張病と悪性緊張病42という2つの用語が生まれた。この致死的となりうる病態とNMSの鑑別は,臨床的にも検査によっても不可能であり,NMSは悪性緊張病の異型である可能性が示唆される43。しかし,ドパミン拮抗薬を使用していない場合はNMSの可能性が除外されると考えられる。
最近のエビデンス,および過去数十年間のエビデンスの大半は,迅速なECTが緊張病の治療として最も有効であると示唆している33, 36, 44-60。ECTに反応する緊張病は,NMS,せん妄性躁病,自閉症の自傷行為,辺縁系脳炎において認められている41。ECTに対する反応は気分障害よりも統合失調症(ないしは抗精神病薬の投与を受けている患者)の方が低い可能性があることが示唆されているが61,ECTは今でも,ベンゾジアゼピン系薬剤を十分に試みても反応しなかった緊張型統合失調症に対する治療選択肢になると考えられている62。悪性緊張病では,十分な全身発作を誘発する刺激を使用してECTの効果を最大にするよう努力する必要がある63。また,身体的な健康も優先すべきであり,特に自律神経の不安定性がみられる場合や精神科的なケアで食事の摂取を管理できない場合には,入院させる必要がある。
抗精神病薬を使用する際には注意深く検討しなければならない。緊張病症状がみられる場合には抗精神病薬をすべからく避けるべきであると推奨する専門家もいるが,アリピプラゾール,リスペリドン,オランザピン,ziprasidone,クロザピンで治療に成功した症例報告もある64-69。クロザピンとオランザピンの使用を支持するエビデンスが最も多いと考えられる。ベンゾジアゼピン系薬剤との併用投与は,それぞれが単独では奏効しない場合に有効となる可能性がある70, 71。
抗精神病薬の使用を検討する場合は,患者の病歴,以前の診断名,抗精神病薬に対する過去の反応,アドヒアランス不良による昏迷の可能性を考慮に入れる。本項の前半に挙げた身体的な疾患によっても緊張病様の臨床像がみられることがあるので,その場合には基礎にある身体疾患(ループス72等)を治療することが重要である。昏迷が抗精神病薬による治療中に生じた場合,NMSの明確な徴候がある場合,筋強剛が自律神経の不安定性を伴う場合は,抗精神病薬は避ける。NMSの可能性が除外され,昏迷が抗精神病薬のアドヒアランス不良によって生じた場合には,早急かつ確実に抗精神病薬を投薬し,ベンゾジアゼピン系薬剤の補助投与を考慮することが推奨される。これは特に,緊張病症状がクロザピンの中止後に生じた場合に該当する可能性があると考えられる25, 73。緊張病は,長期間投与されていたベンゾジアゼピン系薬剤の中断後にも報告されている25。
緊張病性昏迷の治療アルゴリズム74
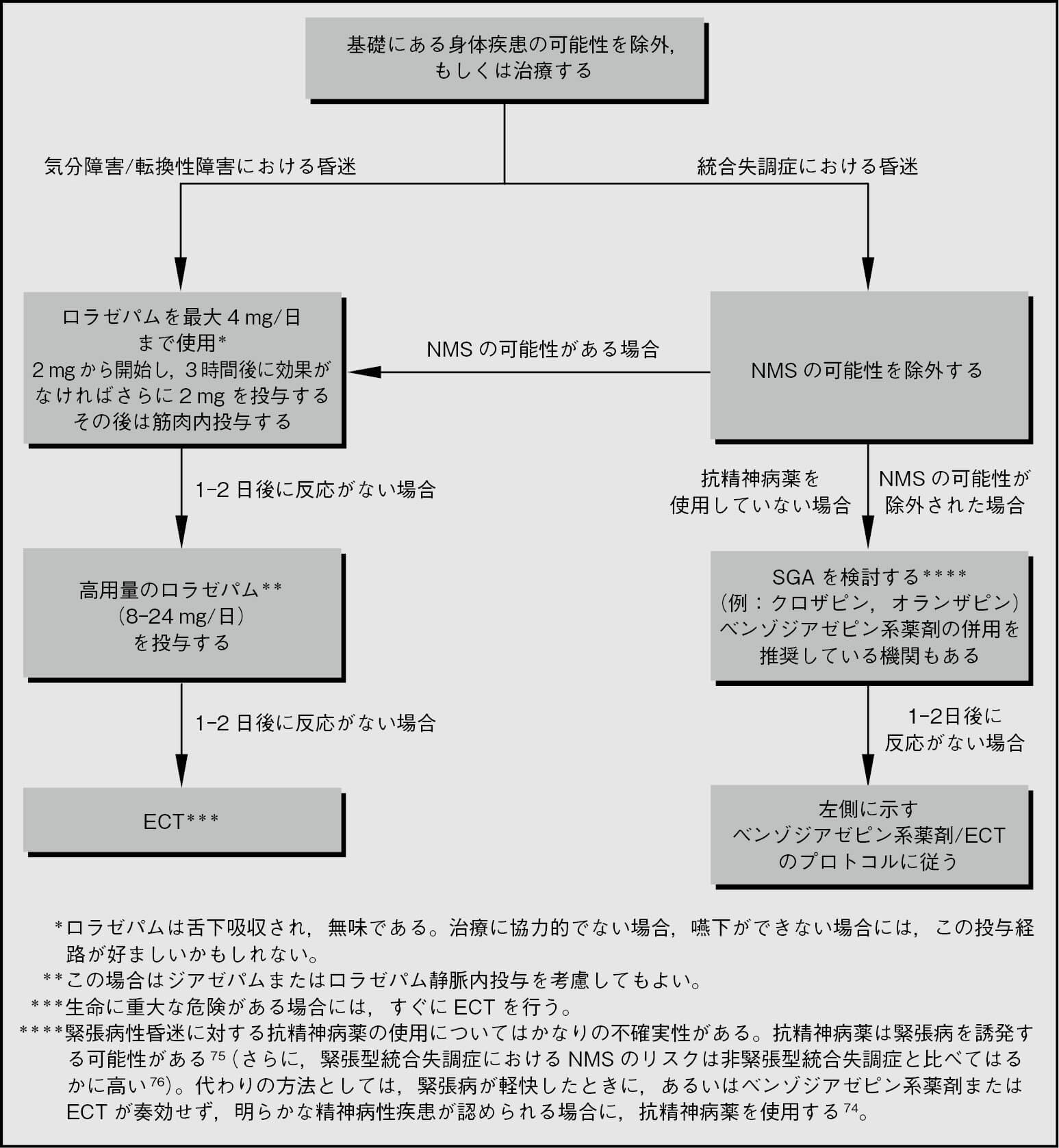
表1.20 緊張病/昏迷に対する治療として報告されているベンゾジアゼピン系以外の薬剤
(順序はアルファベット順であり,序列または判断を示すものではない)
| 抗精神病薬64-69, 77-80 |
|
| 実験的な治療法* 6, 7, 31, 32, 53, 81-86 |
|
*この表に記載した治療薬を使用する際には,一次文献を必ず参照すること。
(長井 信弘)
参照文献
- Morrison JR. Catatonia. Retarded and excited types. Arch Gen Psychiatry 1973; 28:39–41.
- Walther S, et al. Structure and neural mechanisms of catatonia. Lancet Psychiatry 2019; 6:610–619.
- Takacs R, et al. Catatonia in affective disorders. Curr Psychiatry Rev 2013; 9:101–105.
- Mangas MCC, et al. P-167 – catatonia in bipolar disorder. Eur Psychiatry 2012; 27 Suppl 1:1.
- Huang YC, et al. Rapid relief of catatonia in mood disorder by lorazepam and diazepam. Biomed J 2013; 36:35–39.
- Vasudev K, et al. What works for delirious catatonic mania? BMJ Case Rep 2010; 2010.
- Neuhut R, et al. Resolution of catatonia after treatment with stimulant medication in a patient with bipolar disorder. Psychosomatics 2012; 53:482–484.
- Ghaffarinejad AR, et al. Periodic catatonia. Challenging diagnosis for psychiatrists. Neurosciences 2012; 17:156–158.
- Oldham MA, et al. Alcohol and sedative-hypnotic withdrawal catatonia: two case reports, systematic literature review, and suggestion of a potential relationship with alcohol withdrawal delirium. Psychosomatics 2016; 57:246–255.
- Banerjee D. Etizolam withdrawal catatonia: the first case report. Asian J Psychiatr 2018; 37:32–33.
- Fink M. Rediscovering catatonia: the biography of a treatable syndrome. Acta Psychiatr Scand Suppl 2013; 1–47.
- Bartolommei N, et al. Catatonia: a critical review and therapeutic recommendation. J Psychopathology 2012; 18:234–246.
- Lee J. Dissociative catatonia: dissociative-catatonic reactions, clinical presentations and responses to benzodiazepines. Aust N Z J Psychiatry 2011; 45:A42.
- Suzuki K, et al. Hysteria presenting as a prodrome to catatonic stupor in a depressive patient resolved with electroconvulsive therapy. J ECT 2006; 22:276.
- Alwaki A, et al. Catatonia: an elusive diagnosis. Neurology 2013; 80 Suppl 1:P05.127.
- Dhadphale M. Eye gaze diagnostic sign in hysterical stupor. Lancet 1980; 2:374–375.
- Gomez J. Hysterical stupor and death. Br J Psychiatry 1980;136:105–106.
- Petrides G, et al. Synergism of lorazepam and electroconvulsive therapy in the treatment of catatonia. Biol Psychiatry 1997; 42:375–381.
- Mazzone L, et al. Catatonia in patients with autism: prevalence and management. CNS Drugs 2014; 28:205–215.
- Dhossche DM, et al. Catatonia in psychiatric illnesses, in SH Fatemi, PJ Clayton, eds. The medical basis of psychiatry. Totowa, NJ: Humana Press; 2008 :471–486.
- Shetageri VN, et al. Case report: catatonia as a presenting symptom of Wilsons disease. Indian J Psychiatry 2011; 53 Suppl 5:S93–S94.
- Cardinal RN, et al. Psychosis and catatonia as a first presentation of antiphospholipid syndrome. Br J Psychiatry 2009; 195:272.
- Rogers JP, et al. Catatonia and the immune system: a review. Lancet Psychiatry 2019; 6:620–630.
- Pustilnik S, et al. Catatonia as the presenting symptom in systemic lupus erythematosus. J Psychiatr Pract 2011; 17:217–221.
- Lander M, et al. Review of withdrawal catatonia: what does this reveal about clozapine? Trans Psychiatry 2018; 8:139.
- Sienaert P, et al. Adult catatonia: etiopathogenesis, diagnosis and treatment. Neuropsychiatry 2013; 3:391–399.
- Huang TL, et al. Lorazepam reduces the serum brain-derived neurotrophic factor level in schizophrenia patients with catatonia. Prog Neuropsychopharmacol Biol Psychiatry 2009; 33:158–159.
- Fink M, et al. Neuroleptic malignant syndrome is malignant catatonia, warranting treatments efficacious for catatonia. Prog Neuropsychopharmacol Biol Psychiatry 2006; 30:1182–1183.
- Lin CC, et al. The lorazepam and diazepam protocol for catatonia due to general medical condition and substance in liaison psychiatry. PLoS One 2017; 12:e0170452.
- Javelot H, et al. Zolpidem test and catatonia. J Clin Pharm Ther 2015; 40:699–701.
- Bastiampillai T, et al. Treatment refractory chronic catatonia responsive to zolpidem challenge. Aust N Z J Psychiatry 2016; 50:98.
- Peglow S, et al. Treatment of catatonia with zolpidem. J Neuropsychiatry Clin Neurosci 2013; 25:E13.
- Bush G, et al. Catatonia. II: Treatment with lorazepam and electroconvulsive therapy. Acta Psychiatr Scand 1996; 93:137–143.
- Rosebush PI, et al. Catatonia: re-awakening to a forgotten disorder. Mov Disord 1999; 14:395–397.
- Ungvari GS, et al. Lorazepam for chronic catatonia: a randomized, double-blind, placebo-controlled cross-over study. Psychopharmacology 1999; 142:393–398.
- Dutt A, et al. Phenomenology and treatment of Catatonia: a descriptive study from north India. Indian J Psychiatry 2011; 53:36–40.
- Gibson RC, et al. Benzodiazepines for catatonia in people with schizophrenia and other serious mental illnesses. Cochrane Database Syst Rev 2008; CD006570.
- Luchini F, et al. Catatonia and neuroleptic malignant syndrome: two disorders on a same spectrum? Four case reports. J Nerv Ment Dis 2013; 201:36–42.
- Mishima T, et al. [Diazepam-responsive malignant catatonia in a patient with an initial clinical diagnosis of neuroleptic malignant syndrome: a case report]. Brain Nerve 2011; 63:503–507.
- Rodriguez S, et al. Neuroleptic malignant syndrome or catatonia? A case report. J Crit Care Med 2020; 6:190–193.
- Fink M. Expanding the catatonia tent: recognizing electroconvulsive therapy responsive syndromes. J Ect 2020 : [Epub ahead of print].
- Mann SC, et al. Catatonia, malignant catatonia, and neuroleptic malignant syndrome. Curr Psychiatry Rev 2013; 9:111–119.
- Taylor MA, et al. Catatonia in psychiatric classification: a home of its own. Am J Psychiatry 2003; 160:1233–1241.
- Cristancho P, et al. Successful use of right unilateral ECT for catatonia: a case series. J Ect 2014; 30:69–72.
- Philbin D, et al. Catatonic schizophrenia: therapeutic challenges and potentially a new role for electroconvulsive therapy? BMJ Case Rep 2013; 2013.
- Takebayashi M. [Electroconvulsive therapy in schizophrenia]. Nihon Rinsho 2013; 71:694–700.
- Oviedo G, et al. Trends in the administration of electroconvulsive therapy for schizophrenia in Colombia: Descriptive study and literature review. Eur Arch Psychiatry Clin Neurosci 2013; 263 Suppl 1:S98.
- Pompili M, et al. Indications for electroconvulsive treatment in schizophrenia: a systematic review. SchizophrRes 2013; 146:1–9.
- Ogando Portilla N, et al. Electroconvulsive therapy as an effective treatment in neuroleptic malignant syndrome: purposely a case. Eur Psychiatry 2013; 28 Suppl 1:1.
- Unal A, et al. Effective treatment of catatonia by combination of benzodiazepine and electroconvulsive therapy. J Ect 2013; 29:206–209.
- Kaliora SC, et al. The practice of electroconvulsive therapy in Greece. J ECT 2013; 29:219–224.
- Girardi P, et al. Life-saving electroconvulsive therapy in a patient with near-lethal catatonia. Riv Psichiatr 2012;47:535–537.
- Kumar V, et al. Electroconvulsive therapy in pregnancy. Indian J Psychiatry 011; 53 Suppl 5:S100–S101.
- Weiss M, et al. Treatment of catatonia with electroconvulsive therapy in adolescents. J Child Adolesc Psychopharmacol 2012; 22:96–100.
- Bauer J, et al. Should the term catatonia be explicitly included in the ICD-10 description of acute transient psychotic disorder F23.0? Nord J Psychiatry 2012; 66:68–69.
- Mohammadbeigi H, et al. Electroconvulsive therapy in single manic episodes: a case series. Afr J Psychiatry 2011; 14:56–59.
- Dragasek J. [Utilisation of electroconvulsive therapy in treatment of depression disorders]. Psychiatrie 2011; 15:1211–1219.
- Sienaert P, et al. A clinical review of the treatment of catatonia. Front Psychiatry 2014; 5:181.
- Luchini F, et al. Electroconvulsive therapy in catatonic patients: efficacy and predictors of response. World J Psychiatry 2015; 5:182–192.
- Lloyd JR, et al. Electroconvulsive therapy for patients with catatonia: current perspectives. Neuropsychiatr Dis Treat 2020; 16:2191–2208.
- Van Waarde JA, et al. Electroconvulsive therapy for catatonia: treatment characteristics and outcomes in 27 patients. J Ect 2010; 26:248–252.
- Jain A, et al. Catatonic Schizophrenia. StatPearls. Treasure Island (FL): statPearls Publishing Copyright © 2020, StatPearls Publishing LLC. 2020.
- Kellner CH, et al. Electroconvulsive therapy for catatonia. Am J Psychiatry 2010; 167:1127–1128.
- Van Den EF, et al. The use of atypical antipsychotics in the treatment of catatonia. Eur Psychiatry 2005; 20:422–429.
- Caroff SN, et al. Movement disorders associated with atypical antipsychotic drugs. J Clin Psychiatry 2002; 63 Suppl 4:12–19.
- Guzman CS, et al. Treatment of periodic catatonia with atypical antipsychotic, olanzapine. Psychiatry Clin Neurosci 2008; 62:482.
- Babington PW, et al. Treatment of catatonia with olanzapine and amantadine. Psychosomatics 2007; 48:534–536.
- Bastiampillai T, et al. Catatonia resolution and aripiprazole. Aust N Z J Psychiatry 2008; 42:907.
- Strawn JR, et al. Successful treatment of catatonia with aripiprazole in an adolescent with psychosis. J Child Adolesc Psychopharmacol 2007; 17:733–735.
- Spiegel DR, et al. A case of schizophrenia with catatonia resistant to lorazepam and olanzapine monotherapy but responsive to combination treatment: is it time to consider using select second-generation antipsychotics earlier in the treatment algorithm for this patient type? Clin Neuropharmacol 2019; 42:57–59.
- Cevher Binici N, et al. Response of catatonia to amisulpride and lorazepam in an adolescent with schizophenia. J Child Adolesc Psychopharmacol 2018; 28:151–152.
- Grover S, et al. Catatonia in systemic lupus erythematosus: a case report and review of literature. Lupus 2013; 22:634–638.
- Bilbily J, et al. Catatonia secondary to sudden clozapine withdrawal: a case with three repeated episodes and a literature review. Case Rep Psychiatry 2017; 2017:2402731.
- Rosebush PI, et al. Catatonia and its treatment. Schizophr Bull 2010; 36:239–242.
- Caroff SN, et al. Movement disorders induced by antipsychotic drugs: implications of the CATIE schizophrenia trial. Neurol Clin 2011; 29:127–148, viii.
- Funayama M, et al. Catatonic stupor in schizophrenic disorders and subsequent medical complications and mortality. Psychosom Med 2018; 80:370–376.
- Voros V, et al. [Use of aripiprazole in the treatment of catatonia]. NeuropsychopharmacolHung 2010; 12:373–376.
- Yoshimura B, et al. Is quetiapine suitable for treatment of acute schizophrenia with catatonic stupor? A case series of 39 patients. Neuropsychiatr Dis Treat 2013; 9:1565–1571.
- Todorova K. Olanzapine in the treatment of catatonic stupor – two case reports and discussion. Eur Neuropsychopharmacol 2012; 22 Suppl 2:S326.
- Prakash O, et al. Catatonia and mania in patient with AIDS: treatment with lorazepam and risperidone. Gen Hosp Psychiatry 2012; 34:321–326.
- Daniels J. Catatonia: clinical aspects and neurobiological correlates. J Neuropsychiatry Clin Neurosci 2009;21:371–380.
- Obregon DF, et al. Memantine and catatonia: a case report and literature review. J Psychiatr Pract 2011; 17:292–299.
- Hervey WM, et al. Treatment of catatonia with amantadine. Clin Neuropharmacol 2012; 35:86–87.
- Consoli A, et al. Lorazepam, fluoxetine and packing therapy in an adolescent with pervasive developmental disorder and catatonia. J Physiol Paris 2010; 104:309–314.
- Lewis AL, et al. Malignant catatonia in a patient with bipolar disorder, B12 deficiency, and neuroleptic malignant syndrome: one cause or three? J Psychiatr Pract 2009;15:415–422.
- Padhy SK, et al. The catatonia conundrum: controversies and contradictions. Asian J Psychiatr 2014; 7:6–9.